BMI and Pregnancy Success in Gestational Carriers
“These show notes provide more scientific details than the podcast. If you remain curious, please read on! ”
This retrospective case-control study is the first to compare pregnancy and live birth rates in gestational carriers vs. the “generally infertile.”
Study Background
WHAT
Does Body Mass Index (BMI) impact the success of an IVF cycle in a gestational carrier?
WHY
Increasing numbers of gestational carriers carrying IVF babies
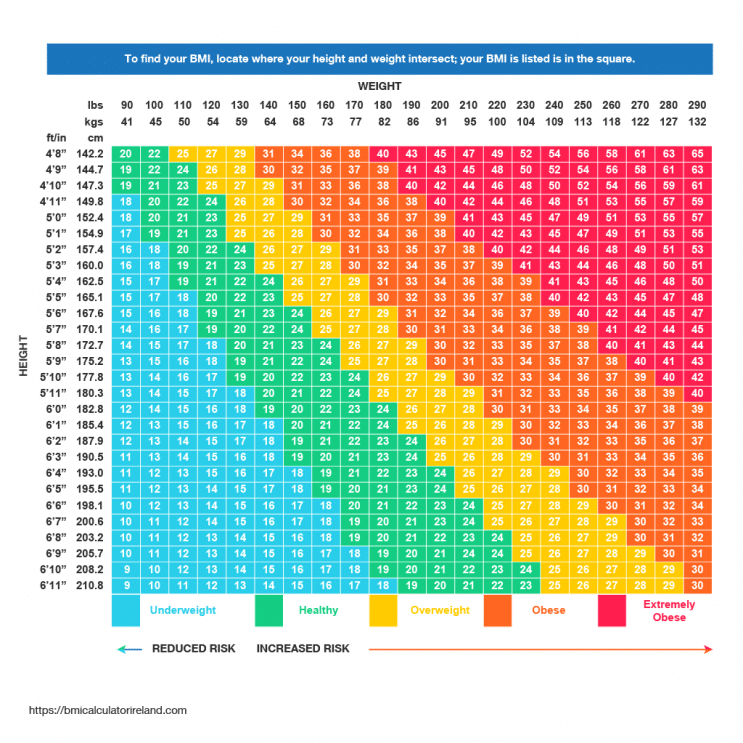
Global pandemic of obesity (per the CDC and the WHO, defined as BMI > 29.9)
Higher BMI = higher risks of negative outcomes to mother and baby
Higher BMI = unknown risks to IVF processes
WHERE
IVF completed at a private fertility center in Toronto, Ontario, Canada
Pregnancy information located in “Better Outcomes Registry & Network” (BORN) database
WHEN
2003-2016
WHO
Gestational Carriers as test group and generally infertile as control group
N = 188 in each group
No age exclusions
Diagnosis exclusions were repeat implantation failure, repeat pregnancy loss, or thin endometrium before embryo transfer
Pre-transfer luteal support was “similar” for all cycles per an unspecified clinic protocol
HOW
1:1 gestational carrier to control match by BMI and treatment year
Retrospective review
clinical charts on medical history
patient self-reported lifestyle factors
pregnancy outcomes
2003-2008, directly contacted patients about birth information
2009 onwards, searched BORN database
Defined primary outcomes - clinical pregnancy, life birth, miscarriage rates
Defined secondary outcomes - pregnancy complications
Extensive statistics
utilized G*power program (version not stated)
alpha of 0.05, Beta of 0.80 and one degree of freedom
sufficient power from 65-126 cycles in each group
Results
BMI did not affect pregnancy, miscarriages, or live births
More gestational carriers became pregnant and gave birth in normal, overweight, and obese groups; no statistically significant differences in morbidly obese
No statistically significant differences in miscarriage rates (after Holm-Bonferroni correction to lower risk of false positive results)
No statistically significant difference in pre-transfer endometrial thickness
No statistically significant differences in embryo characteristics (quality, quantity, day of transfer)

BMI = Body Mass Index; GC = Gestational Carrier; SD = Standard Deviation
There were no statistically significant differences between the groups, although there was a trend towards more morbidly obese women in the “generally infertile” control group.
Authors’ Thoughts
Expected gestational carriers to be younger with more favorable birth records (why selected as carriers), higher pregnancy and birth rates consistent with prior studies
Study strengths:
Increased ability to detect statistical differences by testing outcomes (pregnancy, birth, etc.) as both continuous and as binary variables
By using Holm-Bonferroni method to look at multiple hypotheses, eliminated the falsely positive difference detected in miscarriage rates.
Study limitations:
small sample size
one fertility center
Study results do not clarify if obesity affects results of IVF treatments
This Pharmacist’s Thoughts
Differences at baseline, all statistically significant (p < 0.05)
Gestational carriers younger than controls (age 31.8 years vs. 37.3 years)
Age of source of oocytes (eggs) younger in gestational carriers than controls (age 28.6 years vs. 33.7 years)
Gestational carriers had more previous pregnancies and deliveries
Gestational carriers reported taking more psychiatric medications (16.0% vs. 6.2%)
Generally infertile controls reported lifestyles less conducive to pregnancy
18.6% reported lack of exercise vs. 3.1% of gestational carriers
5.6% report current recreational drug use vs. 1.1% of gestational carriers
Since BMI does not distinguish the density of muscle mass, is BMI the optimal measurement to capture and measure the obesity in this population?
Would different embryo protocols make a difference?
More gestational carriers transferred Day 5 embryos, more controls transferred Day 3 embryos
Primarily fresh embryo transfer (~90%), would there be detectable differences in a large study using primarily frozen embryos?
Was all data reliably located? Contacting patients directly for 2003-2008 outcomes introduces risk of recall bias + introduces inconsistencies in data collection over entire study period
The study did not note patient race or ethnicity data- are there subgroups where the outcomes may be different based on these demographics?
Conclusions
The study results should not lead to changes in selecting gestational carriers. A prospective multi-site study, with women closely matched between groups, would bolster the results of this study.
Currently, ASRM does not recommend excluding women from being gestational carriers based on BMI alone. Given that BMI might not be the best predictor of negative outcomes associated with obesity, future studies should include alternative markers of obesity, such as waist circumference or % body fat.
Resources
Abramowitz MK, Hall CB, Amodu A, Sharma D, Androga L, Hawkins M. Muscle mass, BMI, and mortality among adults in the United States: A population-based cohort study [published correction appears in PLoS One. 2018 May 24;13(5):e0198318]. PLoS One. 2018;13(4):e0194697. Published 2018 Apr 11. doi:10.1371/journal.pone.0194697
Adult Overweight and Obesity. Centers for Disease Control and Prevention website. https://www.cdc.gov/obesity/adult/index.html. Accessed August 25, 2020
Body Mass Index (BMI). Centers for Disease Control and Prevention website. https://www.cdc.gov/healthyweight/assessing/bmi/index.html. Accessed August 25, 2020.
Fuchs Weizman N, Defer MK, Montbriand J, Pasquale JM, Silver A, Librach CL. Does body mass index impact assisted reproductive technology treatment outcomes in gestational carriers. Reprod Biol Endocrinol. 2020;18(1):35. Published 2020 May 2. doi:10.1186/s12958-020-00602-2
Gestational Carrier (Surrogate). American Society for Reproductive Medicine. https://www.reproductivefacts.org/news-and-publications/patient-fact-sheets-and-booklets/documents/fact-sheets-and-info-booklets/gestational-carrier-surrogate/ Accessed August 25, 2020.
Made in Boise. https://www.pbs.org/independentlens/films/made-in-boise/. Accessed August 25, 2020.
Practice Committee of the American Society for Reproductive Medicine and Practice Committee of the Society for Assisted Reproductive Technology. Electronic address: ASRM@asrm.org; Practice Committee of the American Society for Reproductive Medicine and Practice Committee of the Society for Assisted Reproductive Technology. Recommendations for practices utilizing gestational carriers: a committee opinion. Fertil Steril. 2017;107(2):e3-e10. doi:10.1016/j.fertnstert.2016.11.007